

|
|
he coronavirus disease 2019 (COVID-19) pandemic is unprecedented in modern times, bringing enormous human, social, and economic disruption. As of March 18, 2020, over 215,000 cases have been reported worldwide. China, the origin of the epidemic, represents over 80,000 of these cases, but extraordinary action to lock down entire cities resulted in a remarkable decrease in the number of new cases, though they must remain vigilant to prevent a spike in new infections. Now, an alarming number of COVID-19 diagnoses have been confirmed in 170 countries around the world, with the most affected countries being Italy, Iran, Spain, Germany, South Korea, France, the United Kingdom, and the United States.
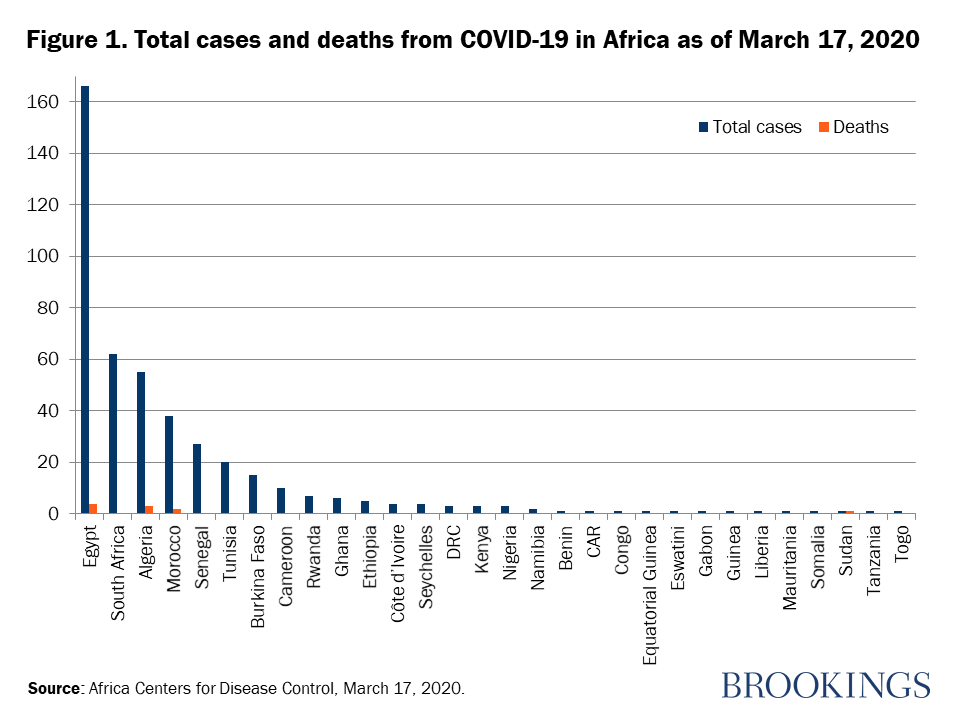
For Africa, where most countries have relatively weak health systems, the slow arrival of COVID-19 bought precious time to prepare. In collaboration with the World Health Organization and the Africa Centers for Disease Control (CDC), national governments have been mobilizing precautionary measures, most notably flight restrictions, enhanced screening at international airports, isolation, and contact tracing, as well as training of health personnel in anticipation of a potential epidemic. Nevertheless, 443 total cases have been reported in 30 African countries, with 10 deaths reported in four as of March 17 (Figure 1).
Since most African countries are within the containment phase of the epidemic curve, time is of the essence, and urgent action to prevent an epidemic should be the overriding objective. African leaders should learn from Asia and Europe. Here are four early lessons to heed in responding to the ongoing outbreak and preparing for future ones.
1. Act with speed and thoroughness to prioritize prevention of an epidemic. Early action consisting of case identification, tracing and containment measures, clear and transparent communication with the public, and resource mobilization is critical precisely because most health systems on the continent are fragile and likely unable to absorb the shock of a global pandemic, especially the management of severe cases. Lessons from China, Singapore, Taiwan, and Hong Kong show that swift action must be taken as early as possible—even at the risk of seeming to overreact—as this strategy can greatly influence the trajectory of new infections. Importantly, the astonishing trajectory of the epidemic in Europe confirms that, in the absence of drastic action, even the best health systems in the world might crumble under the weight of this epidemic.
2. Heed lessons from Africa’s history of infectious disease epidemics. The 2014 Ebola outbreak led some countries to create or empower national public health institutes to focus on disease preparedness and responsiveness in the case of an epidemic. Liberia and the Democratic Republic of the Congo, for example, have rapidly erected facilities for screening and diagnosis, and training programs to help doctors and nurses recognize the symptoms of COVID-19. The Nigeria Centers for Disease Control (NCDC) was already handling an ongoing Lassa fever outbreak, which has a much higher mortality rate (23 percent) compared to what is estimated for coronavirus (3 percent). The NCDC is now actively addressing the COVID-19 emergency response, with the credibility of an independent institution run by experts working in the public interest and independent of political interference. For the current outbreak, many African countries have set up a multidisciplinary task force to direct the emergency response to COVID-19. As this epidemic runs its course, these teams must evolve into pillars of collaboration for the setting up of national public health institutes run by experts empowered with the necessary financial and human resources. Epidemic preparedness must begin before the next outbreak. Investments in public health and preparedness by one country have an enormous impact on the capacity of the whole region to manage a pandemic.
3. Leverage big data, information technology, and predictive modeling to anticipate the health and economic impact of the epidemic and to guide decisionmaking. Africa has the youngest population in the world with a median age of 18 years, compared to 41 years in Europe. While the mortality of COVID-19 varies from country to country, the age and health of the population seem to be major factors, with the highest mortality rates recorded in patients aged above 60 years old. Notably, about 3 percent of sub-Saharan Africa’s population is over 65 years old. Then again, Africa also has the highest burden of infectious diseases and related comorbidities whose impact on the capacity of the immune system to fight off a COVID-19 infection is unclear. Given the different demographics, the use of European or Asian prediction models is clearly inappropriate in the African context, and Africa must develop its own capacity for predictive modeling to guide decisions on the containment measures to undertake.
On the economic front, the high mobile penetration and connectivity rates across the continent allow for leveraging of telecoms data as an early reporting tool to gather real-time data for informed decisionmaking. With a penetration rate of 105 percent, Kenya’s sophisticated mobile money platform can be modeled to predict the economic impact of specific interventions in the formal and informal sectors, providing household level data in the African context, and guiding decisions on mitigation strategies that are likely to have the greatest impact.
4. In our globalized world, prioritize partnerships. African governments must urgently increase their investments in scientific research and medical infrastructure, and proactively seek partnerships at the continental and global levels. Scientists at the Pasteur Institute of Dakar are already leading the way, working with a biotech laboratory in the United Kingdom to produce a cheap, rapid diagnostic test for COVID-19, manufactured in Senegal, that could reduce diagnosis time from 4 hours to 10 minutes. Scientists at the NCDC already shared with the global community the viral genome of the first confirmed case of SARS-CoV-2 from Africa, contributing to a growing body of research and disease control that benefits everyone. Importantly, such collaborations help equalize global health inequities by ensuring that solutions developed through global collaborations are locally available. In the days ahead, close collaboration with European partners will also be essential in anticipating and accelerating the implementation of potential solutions.
For now, Africa’s main vulnerability to the COVID-19 pandemic remains European provenance. This reality has put to question a global system that is predicated on infectious diseases originating in Africa going towards the West. With the tables turned, Africa has had to take a more proactive role in learning from the successes and failures of Asian, European, and American partners in shaping her own response to COVID-19 to protect African populations, minimize case importation, and avert a large-scale epidemic.









{kind=link}